


Healing knows no gender: Still forbidden male gynecologists in India have to face
In an area built on sympathy and precision, why does the penis still come on the way?


In a country where conversations about women’s health are already immersed in discomfort and silence, the idea of a male gynecologist increases eyebrows. Despite the stories of decades of medical progress and countless success from male doctors in the region, many women in India still hesitate or refuse to consult them. Cultural conditioning, concerns of secrecy, and a sense of strange have made it a stigma running in clinics and hospitals across the country.
To understand the roots of this hesitation and how it affects both patients and physicians, we have Dr. Smate Patel, endometriosis specialist, spoke to an endometriosis specialist at the Meflower Women’s Hospital in Ahmedabad. With years of experience in one of India’s most sensitive medical specialties, he provides navigating bias, building faith with patients, and a unique perspective about calm but significant changes that it is happening in the approach-especially among the small, urban women.
In a country where conversations around women’s health are still considered taboo in many circles, Indian women are actually how comfortable with consulting a male gynecologist, what changes have you seen over time?
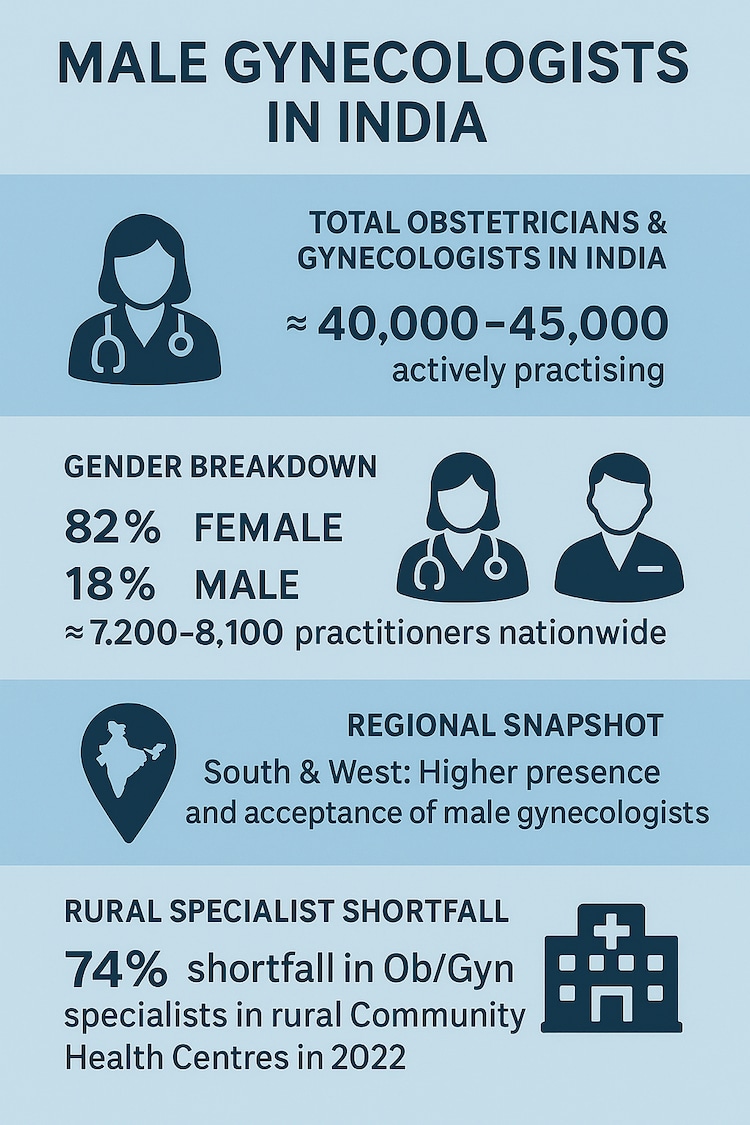
In India, many women still prefer female gynecologists, especially for consultation and intimate exams-as it helps them make them feel more comfortable and safe. However, when it comes to surgery, especially in complex cases such as endometriosis, the experience often overtakes gender preference. We have seen that many patients voluntarily opted for male surgeons when they know that those experts are in hands. Eventually healing does not know any gender.
In the mefloor, we have installed a system that respects both comfort and ability: female gynecologists participate in all consultations, while our old male surgeons take care of surgery. This integrated system has worked to create confidence and provide the best results. Finally, the big problem gender-this is not wrong diagnosis. So many women still tolerate because endometriosis is not diagnosed or seriously treated. That is what we want to change: with both sympathy and expertise.
Despite your medical expertise, have you ever faced resistance or doubt from patients or their families
Are you a male gynecologist? Have you faced resistance as a male gynecologist?
Yes, of course and I understand that. In a feature that requires deep confidence and emotional security, women clearly prefer to see female physicians, especially in the beginning. My approach is the first rest: all counseling and follow -up female gynecologists. When patients listen to their care and feel safe, they are ready to take the next step, whether it is an advanced nature surgery or treatment, is usually taken care of by our male employees. The real issue gender-this is not a gap in diagnosis and treatment. A lot of women are brushed, misrepresented, or treated symptomally. We focus on listening with intensity, teaching patients and treating the source with accuracy. When your care is guided by compassion and results, trust naturally.
Why is endometriosis so low in India?
Endometriosis is a chameleon. It manifests in the form of symptoms such as cramps, fatigue, swelling, or back pain during the period that are familiar and is rejected very often as “normal” by doctors and patients. This deep sitting cultural insignificance of women’s pain is one of the greatest obstacles for early diagnosis.
It takes an average of 7 to 10 years to accurately diagnose a woman. There are some reasons clinical boundaries-altrasound still dominates a large extent, and it usually recalls deep and non-marital endometriosis. Although MRI is better in detecting, it is highly dependent on an eye that has been trained, and, regret, many of these radiologists are not trained to take microscopic signs.
 than you think")
The worst, women are often called, “all this is in your head,” or there is no clear diagnosis on the cycle of pain and hormone tablets. It contributes to years of unmarried disease, emotional turmoil and avoidable damage. In the meflower, we have labeled many women with “unexplained infertility” or “chronic pelvic pain”, only to search for extensive endometriosis only later. It is important to increase awareness between both patients and general physicians as to pursue a clinical equipment.
How does endometriosis affect fertility and what myths do you see?
Endometriosis often quietly damages fertility. About half of all women facing infertility can contain unknown endometriosis. This is not a surface problem-this condition causes pelvic adhesions, obstructs the fallopian tubes, forms ovarian ulcers (also known as chocolate ulcers), and interfere with the uterine environment in such a way that the fertilization and implantation become impossible. Even the uterus can contract itself improperly, interfering with fetal implantation.
What is most inconsistent is the perseverance of myths. “If your period is not painful, it is not endometriosis,” or “just a child-it will do it.” These diagnoses postpon diagnosis and treatment, resulting in irreparable disadvantages. Worse, many women attempt many unsuccessful IVF efforts without sometimes correcting the underlying endometriosis. IVF is not a magic solution-it only works best when the disease is initially treated properly. Therefore we attack early diagnosis, complete care, and cause of the disease, not just symptoms or quick solutions.
Given the increasing awareness of endometriosis in India, but still limited understanding, how accessible and inexpensive are fertility treatments for women struggling with this situation?
Breeding clinics are common nowadays, but very few people have an endometriosis-causing experience treating infertility. Central treatment for such patients is not just to remove IVF-It disease. Here in the mefloor, with more than 20,000 endometriosis surgery under our belt, our primary purpose is to always return natural fertility. When surgery is done correctly, many patients become pregnant spontaneously. And for those who still need IVF, success rate is much better after treatment. For the right treatment at the right time, it all matters. This is not much process-this is the right way.